|
Although HIV infection affects people from all ethnic groups,
genders, ages, and income levels, some groups have been significantly
affected by the AIDS epidemic. These groups have included
men who have sex with men, injecting drug users, people with
hemophilia, women, and people of color. The difference with
the grief process associated with HIV and AIDS can be the
social and emotional issues associated with contracting the
disease. The following information details how these different
populations may be uniquely affected by the AIDS epidemic.
Men Who Have Sex With Men
Despite gains in human rights, our American society still
has issues with men who have sex with men. Grief may not be
validated when relationships are considered "unacceptable."
An example of this may be the reaction of churches to those
who are living with, or have families living with AIDS. Many
congregants report that they do not get the support they need
from their church families because of the stigma attached
to HIV, AIDS and to men who have sex with men.
Self-esteem issues and psychological issues (including depression,
anxiety, diagnosed mental illness and risk-taking behaviors)
may also complicate the lives of these men. Additionally,
there are the issues with HIV-negative men who have sex with
men. Most of the attention, resources and services are focused
on HIV-positive men. As with any behavior change people can
become "tired" with safer sex messages, and may make choices
that place them at risk. Some may feel that HIV infection
is inevitable (although it is not) and purposely engage in
unprotected sex.
Injecting Drug Users
American society also has issues with illegal drug use and
the way we view marginalized individuals such as those in
poverty and the homeless. Drug users are also stigmatized.
People who continue to use injecting drugs, despite warnings
and information about risks, may be viewed by some as "deserving"
their infection. However, it is important to remember that
addiction is an illness and rarely does "just say no" work
to stop the addiction; indeed it trivializes the seriousness
of addiction.
Harm reduction measures like syringe exchange programs, have
been proven to reduce the transmission of blood-borne pathogens
like HIV, HBV, and HCV. These programs are controversial because
some people believe that providing clean needles and a place
to exchange used needles constitutes "approval" of injection
drug use.
In addition to poverty, self-esteem issues and psychological
issues, including depression, anxiety, diagnosed mental illness
and risk-taking behaviors, may also complicate the lives of
injection drug users. The desire to stop using illegal drugs
and the ability to do so may be very far apart. The reality
about inpatient treatment facilities is there are very few
spaces available for the demand. Many injecting drug users
are placed on "waiting lists" when they want treatment, and
by the time there is a place for them, the individual may
be lost to follow-up.
People with Hemophilia
Hemophiliacs lack the ability to produce certain blood clotting
factors. Before the advent of antihemophilic factor concentrates
(products like "factor VIII" and "factor IX," which are clotting
material pooled out of donated blood plasma), hemophiliacs
could bleed to death. These concentrates allowed hemophiliacs
to receive injections of the clotting factors that they lacked,
which in turn allowed them to lead relatively normal lives.
Unfortunately, because the raw materials for these concentrates
came from donated blood, many hemophiliacs were infected with
HIV prior to the advent of blood testing.
During the 1980's, prior to routine testing of the blood
supply, 90% of severe hemophiliacs contracted HIV and/or HCV
through use of these products. There is anger within this
community because there is evidence to show that the companies
manufacturing the concentrates knew their products might be
contaminated, but continued to distribute them anyway.
While some people considered hemophiliacs to be "innocent
victims" of HIV, there had been significant discrimination
against them. The Ryan White Care Act, funding HIV services,
and the Ricky Ray Act, which provides compensation to hemophiliacs
infected with HIV, were both named after HIV-positive hemophiliacs
who suffered significant discrimination (arson, refusal of
admittance to grade school, etc.) in their hometowns.
Women
Certain strains of HIV may infect women more easily. The
strain of HIV present in Thailand seems to transmit more easily
to women through sexual intercourse.
Researchers believe that women and receptive partners are
more easily infected with HIV, compared to the insertive partner.
Receptive partners are at greater risk for transmission of
any sexually transmitted disease, including HIV.
Women infected with HIV are at increased risk for a number
of gynecological problems, including pelvic inflammatory disease,
abscesses of the fallopian tubes and ovaries, and recurrent
yeast infections. Some studies have found that HIV-infected
women have a higher prevalence of infection with the human
papilloma virus (HPV). Cervical dysplasia is a precancerous
condition of the cervix cause by certain strains of HPV. Cervical
dysplasia in HIV-infected women often becomes more aggressive
as the woman's immune system declines. This may lead to invasive
cervical carcinoma, which is an AIDS-indicator condition.
It is important for women with HIV to have more frequent Pap
tests.
Several studies have shown that women with HIV in the U.S.
receive less health care services and HIV medications, compared
to men. This may be because women aren't diagnosed or tested
as frequently as men.
The number of women with HIV (human immunodeficiency virus)
infection and AIDS has been increasing steadily worldwide.
By the end of 2003, according to the World Health Organization
(WHO), 19.2 million women were living with HIV/AIDS worldwide,
accounting for approximately 50 percent of the 40 million
adults living with HIV/AIDS (NIAID, 2004).
Figure 1. Proportion of AIDS Cases among
Female Adults and Adolescents, by Transmission Category 2003-United
States (CDC, 2005e). 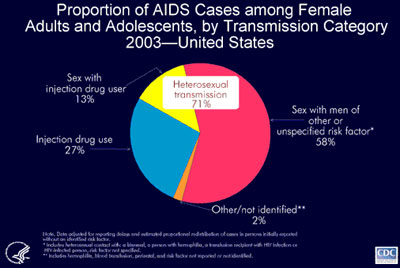
CDC estimates that 71% of the 11,498 AIDS cases
diagnosed among female adults and adolescents in 2003 can
be attributed to heterosexual transmission: 13% of these cases
are from heterosexual contact with an injection drug user
and 58% from sexual contact with high-risk partners such as
bisexual men or HIV-infected men with unidentified risk factors
(CDC, 2005e). Of the cases in female adults and adolescents,
27% were attributed to injection drug use and 2% to other
or unidentified risk factors (CDC, 2005e).
Worldwide, more than 90 percent of all adolescent
and adult HIV infections have resulted from heterosexual intercourse.
Women are particularly vulnerable to heterosexual transmission
of HIV due to substantial mucosal exposure to seminal fluids.
This biological fact amplifies the risk of HIV transmission
when coupled with the high prevalence of non-consensual sex,
sex without condom use due to some women's inability to negotiate
safer sex practices with their partners, and the unknown and/or
high-risk behaviors of their partners (NIAID, 2004).
Younger women are also increasingly being diagnosed
with HIV infection, particularly among African-Americans and
Hispanics. Through December 2002, women aged 25 and younger
accounted for 9.8 percent of the female AIDS cases reported
to CDC (NIAID, 2004).
HIV disproportionately affects African-American
and Hispanic women. Together they represent less than 25 percent
of all U.S. women, yet they account for more than 82 percent
of AIDS cases in women (NIAID, 2004).
Women suffer from the same complications of
AIDS that afflict men but also suffer gender-specific manifestations
of HIV disease, such as recurrent vaginal yeast infections
and severe pelvic inflammatory disease, which increase their
risk of cervical cancer. Women also exhibit different characteristics
from men for many of the same complications of antiretroviral
therapy, such as metabolic abnormalities (NIAID, 2004).
Frequently, women with HIV infection have great
difficulty accessing healthcare; they may postpone taking
medication, or going to their own medical appointments because
of the heavy burden of caring for children and other family
members who may also be HIV-infected. They often lack social
support and face other challenges that may interfere with
their ability to adhere to treatment regimens (NIAID, 2004).
Women (and also men) may fear disclosing their HIV status
to others, out of fear of losing their jobs, housing, or other
forms of discrimination. Single parents with HIV may feel
particularly fearful because of their lack of support.
Many women have problems with lack of transportation,
lack of health insurance, limited education and low income.
They may have child-care problems that prevent them from going
to medical appointments.
Many women who have HIV infection do not consider
this to be their "worst problem". Their symptoms may be mild
and manageable for many years. Meanwhile, they may have more
pressing concerns, such as their income, housing, access to
medical care, possible abusive relationships, and concerns
about their children.
Continue on to Select Populations
and HIV/AIDS, Con't.
|